C22H29FO5 – the wonder drug
As it is nearly 40 years since I was awarded a BA(Hons) in Chemistry, I think I can be forgiven for not being able to give the modern name for dexamethasone. This is the drug announced this week used to treat patients with Covid-19 resulting in reduced deaths for those receiving oxygen or on mechanical ventilators.
Nomenclature has changed since I taught chemistry for five years in the mid-80s. Looking back at the literature of the time it was called 9α-fluoro-16α-methylprednisolone or 6α-methyl-9α-fluoroprednisolone, but either way even having done a biochemistry module I am not sure I would have known it was a steroid derivative of the well-known drug hydrocortisone. One of the main topics I enjoyed was organic chemistry, that of carbon compounds. Looking through the 1,280 pages of Hendrickson, Cram and Hammond’s textbook from 1977 there is no mention of it, despite being used in a clinical way since 1961. To complete the confusion that people often express when I tell them I used to teach chemistry, it is always good to have a chemical structure to describe the compound. Here are two for this drug.

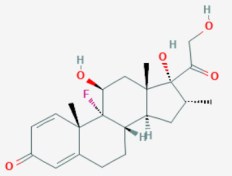
The slightly more modern version on the right shows the different elements hydrogen, oxygen and fluorine as different colours and the methyl (CH3-) structures as a dark triangle. My pharmacy consultant (and wife) Alyson tells me that I was on dexamethasone for a short time in 2012. I was in hospital for 12 weeks (the time we have been locked down now) with a brain abscess, and was given it to reduce the resultant swelling of my brain.
The research on dexamethasone done in British hospitals, with volunteer patients involved in the clinical trials, has been hailed as ground-breaking. The drug has potential to save tens of thousands of lives worldwide. It must be devastating for those who have lost loved ones who may have benefited from it. This and the amazing dedication of the care staff, cleaners, physios, pharmacists, therapists, doctors, nurses, and administrators demonstrate the best of our NHS. As a country and tax payers we need to fund them to the level required. We will have a thorough review and ‘learn the lessons’, but I fear that once ‘real life’ takes over and self-interest resumes its ‘normal life’, we will forget those weeks early on when as one voice we said ‘this can’t be allowed to happen again’.
The whole system needs a thorough rethink. There have been many reviews and reorganisations over the years, and it would be natural for those who work in it to think ‘oh no not again’. The NHS needs rebuilding from the ground up, and possibly renaming. Before Covid-19 I think most people thought of the NHS mainly as the hospitals and local surgeries. In latter years, and certainly during the crisis, there have been concerns that care homes, mental health services, and some social care is linked to the NHS. Many people comment on ‘private business’ not getting involved in our health system as a bad thing. Well I have news for them, much of what we think of are ‘private businesses’. Community pharmacies which I worked in for over 20 years and Alyson has worked in for 40 now, are private limited companies owned mostly by pharmacists but some by medical wholesalers. The same is true of almost every doctor’s surgery who are businesses of doctors setup as a partnership of lead GPs who employ other GPs to help them. These private businesses operate as ‘contractors’ and are paid by Department for Health and Social Care (DHSC), itself only renamed in January 2018. They are paid a rate for their services, whether that’s seeing patients, running clinics or dispensing prescription or carrying out medicine use reviews that is negotiated by their professional bodies with DHSC. It should not be a surprise that negotiating with what is in effect a ‘monopoly’ supplier is not one that leads to mass riches. What does surprise those doctors who visit pharmacies or chat to owners is unlike their partnerships, DHSC pays nothing towards premises or staffing costs of pharmacy businesses, or pay for the holding of large amounts of drug stocks. And don’t even get me on the subject of Dispensing Doctor practices – people who can write a prescription if they have too much stock of a particular drug, or choose the one that’s best for their business rather than the patient.
‘Business’ and the idea of accountability and competition has been part of the health service for many years, and now we have ‘Trusts’ who are independent organisations running services at a local or regional level. They contract to suppliers and surgeries, pharmacies and ‘buy in’ other services from blood and organ donation services, laboratory services and a host of other clinical ones. There are companies who contract for IT projects, finance, property building and maintenance, catering, cleaning etc. This started when I was still in pharmacy 20 years ago and even then I could see the problems of having local GPs on trusts. As with teachers and risk assessments I wrote about in an earlier blog, most GPs are not businesspeople and they can’t be blamed for conflicts of interest between their business and that of patients and other contractors.
Many governments have presided over reforms but the last major one by the coalition government in 2010 and overseen by Andrew Lansley has proven to be disastrous. Even before starting it drew criticism from a lot of areas. The idea of giving even more power to GPs and frontline staff and increased ‘competition’ on one level might seem like a good one, but in reality it led to a mix of systems and lack of any central accountability. The devolving of the social care and public health issues to local government foundered as the secretary of state for health, Jeremy Hunt, cut the budgets under the guise of ‘austerity measures’. The well-publicised ‘scandals’ with Mid Staffordshire NHS Trust and others in care homes can be laid at the lack of oversight on patient safety. The organisation Public Health England (PHE) was formed as a result of abolishing Strategic Health Authorities (SHAs), and at the time several directors warned that this would compromise our ability to ‘fight any future pandemic’. SHA’s would have been able to lead on organising the local response and would have people on the ground able to conduct a ‘track and trace’ system. Andrew Lansley stepped down from government in 2015 and was rewarded for his efforts with a seat in the House of Lords.
Jeremy Hunt was the secretary of health who ignored the results of ‘Operation Cygnus’ in October 2016 used to check the resilience of the NHS to respond to a pandemic (albeit one of influenza). As widely reported at the start of this pandemic, this led to a failure to replenish our stockpiles of PPE, antiviral drugs and ventilators. It is shocking to see him in recent weeks, as the now chair of the parliamentary health and social care select committee, taking the government to task over their failure on issues he was responsible for. When he was elected by MPs to this role in January there was a feeling that this conflict of interest might stop him questioning too much. It’s extraordinary to see the exact opposite happening, but his ability to wipe clean his own responsibility is equally unbelievable.
Andrew Lansley promised a ‘bottom up’ review but ended up with more ‘top down’ structures in place and setting up a whole series of ‘independent bodies’ to monitor things.
Several people have expressed surprise that hospices receive so little funding from DHSC and other government bodies that they have to rely on local fundraising and charitable status to continue. This was put in the spotlight early in the current crisis when fundraising stopped and no provision was forthcoming to help with PPE. If a national health service is supposed to cater for us from ‘cradle to grave’, what has gone so wrong that patients and their families who are facing the real end of the health system are left to donations and sales from charity shops for the provision of care to their loved ones. Another part of the health service that I have experience of, and which has been neglected are rehabilitation units. It seems Covid-19 is an illness that takes a terrible toll on survivors, with months of aftercare needed to even walk again. Many weeks on a ventilator in a medically-induced coma leads to mental health issues as well as physical weakness.
NHS IT provision, which I had some experience of when trying to implement the Electronic Prescription Service (EPS) in our pharmacy branches in 2005/6 was one riven with problems. With the help of our wholesalers and investment in NHS broadband we got all 50 branches setup just as we were sold to the Co-op. Alyson continued working in branch and even now, 14 years on, the system is not fully implemented and looks unlikely to be any time soon. Only recently can pharmacists see a very small amount of information held nationally on any patient who comes into their branchwhen they are away from the place they live. I know from personal experience that my local hospital, 15 miles from the one in another county and a separate trust where I was treated for my brain injury, can’t access any of my scans or records. This is why I have a lever arch folder with all my records and several CDs of my scans/x-rays that I can take in should it happen again.
As predicted by my sons in a blog six weeks ago NHS IT, or NHSX as it is now called, was criticised this week for the failure to deliver the NHS Test & Trace app, and are considering reverting to the Google/Apple model. As my chair of district tweeted;
In all the ‘clap for carers’ and accolades given to those in the health and care systems, we shouldn’t fall into the trap of thinking everyone is working for the common good. In an organisation of about 1.5 million people there will be some ‘bad apples’ and strong management and administration supported by decent pay and training is needed.
Our National Health service should be as much about prevention and encouragement to live a healthy lifestyle as it is about treating us when we fall ill. The effects of obesity, diabetes, heart disease and respiratory conditions on the death rate from coronavirus demonstrates this need. The savings made from prevention should outweigh the costs of later treatment. Education, as in many things, is vital for health outcomes as is reducing poverty.
Let’s hope the next review takes all of the factors into account and, as I wrote last week, as a country we can fund the necessary changes. Our National Health Service has become a ‘Reactive Illness Programme’ (RIP), and needs to change, and quickly.
Other news this week
- The ‘old normal’ resurfaced in our area this week when 6,000 people attended raves in two separate areas of Manchester on Monday. Several people were stabbed, one girl allegedly raped and local people had to clear up the mess after everyone had left.
- Crime seems to be on the increase (or at least being more reported) and terror is back on our streets with the stabbings in Reading this weekend.
- There is more talk of reducing the social distancing requirements to one metre to get hospitality and self-catering holiday accommodation open.
- Dame Vera Lynn died this week at the age of 103. She was called the ‘forces sweetheart’ during World War Two and had shared her thoughts during the current crisis and her song was echoed in the address to the nation by our Queen when she said ‘we will meet again’.
- The Labour Party review on the reasons for disastrous results in December’s general election was published. It didn’t make comfortable reading for members of the party like me. We must work for Labour to produce policies which chime with the need to do things differently in relation to funding the new health and social care system, tackling poverty, improving education and closing the gap between the wealthy and poorer in society.
- The daily death announced totals continue to fall with the Monday-Friday total this week being 853 down from 1,065 last week (a fall of 20%). The total of deaths at the end of the week was 42,632.
- With numbers seemingly under control in European countries despite some local outbreaks in Germany, I looked again at the statistics on Johns Hopkins site and there are some awful looking graphs in other areas of the world. Here are the graphs for cases in Europe;
These show that we are over the (first?) peak of infections. The story in two countries with presidents who think it is nothing to worry about, and are trying to get their country’s open again is not so hopeful…
and note that the scales on these are tens of thousands rather than the thousands in Europe.
The middle and far east countries are also showing curves which are concerning, with a ‘double peak’ for Iran. The cases are in hundreds but show no signs of decreasing.
- We need to start looking overseas again now that we are getting the UK cases down. There is concern from aid charities that helping less well-off countries will be harder now that the department for international development (DFID) and the UKAid agency has been subsumed into the Foreign Office. A move criticised by three recent former prime ministers from both Conservative and Labour.
- The debate and protests around racism and the ‘Black Lives Matter’ movement continued across the world.
- I was going to write that the demonstrations and actions of climate protestors, similar to the ones for Black Lives Matters with marches and ‘direct action’ had not resurfaced, when yesterday I saw an interview with Greta Thunberg saying that she was looking forward to going back to school in Sweden, and vowing to carry on campaigning.
- Greta’s target for criticism president Donald J Trump was back on the campaign trail with a ‘huge rally’ in Tulsa, Oklahoma where only 6,000 of a possible 19,000 seats were occupied despite over a million applications for tickets. For those who did attend there was little sign of masks or social distancing, and six of the organisers caught the virus. At the time of writing there are reports that Mr Trumps rally had been ‘turned over’ by teens and young people responding to campaigns on the Tik-Tok and K-Pop social media platforms applying for tickets then not turning up. Mr Trump said earlier in the week that a million supporters would come.
How has week 13 been for us?
Unfortunately we have another example of the ‘worst of the NHS’ in our household. Five weeks after Alyson applied to help out NHS 111 with taking phone calls from people who need to speak to a pharmacist, and after three polite chasing emails and responses from the HR team doing the ‘on-boarding’ stating that she will hear ‘in a few days’, there is still no sign of her contract or training plans. She has played her part by taking two more calls on the SOS NHS volunteering app.
We haven’t ventured to ‘non-essential shops’ yet and the crush at the Nike store in London and the lady interviewed in the Primark queue in Manchester who stated that she ‘felt like I’ve won the lottery’ didn’t pursuade us. We did go for another walk in Delamere Forest and had a picnic which was pleasant. The weather meant another postponement of meeting with friends in our garden, but we have a walk planned in a park further afield this week.
I have watched a couple of the Premier League football matches now live on ‘free tv’ and have been surprised how realistic the ‘virtual crowd noise’ is to make them seem more ‘normal’ despite empty stadiums. The online radio commentary I heard for my team Middlesbrough was a sign of the ‘new normal’ being much like the old – we lost 3-0 and are looking at relegation again.
I had my first international Zoom with a call to our subcontractors’ office in India with the person who helps on the IT project I am doing. We have had training sessions with the team from our district who are attending the Methodist Conference in a week’s time. With over 300 representatives, Zoom will be in the form of a webinar where we can only see the person presenting and another speaker who wants to add to the debate. Voting will by the raising of a virtual hand or completing a poll on the screen, so the feedback on numbers should be much quicker than the usual manual count of raised hands in the conference hall. I will write more about this next week. The conference service on Sunday will be at my now ‘virtual home church’ of Methodist Central Hall, Westminster in London.
Keep safe and let’s hope there is a safe further easing of lockdown in the coming week.